
Abstract
Background
Globally, cardiovascular diseases (CVDs) have continued to ravage the human existence through the premature deaths of its workforce. Despite this burden, many studies in Nigeria have focused on determining the prevalence of risk factors which alone are insufficient to assess the risk of future cardiovascular events. Therefore, we determined the pattern and predictors of 10-year risk for CVDs in South-western Nigeria.
Methods
We conducted a cross-sectional study among workers at the local government areas (LGAs) of Oyo State. Using a multi-stage sampling technique, we recruited 260 respondents from the LGA secretariats. A pre-tested, interviewer-administered questionnaire was administered to obtain information on the socio-demographics and behavioural attributes. Lipid analysis, anthropometric, blood pressure, fasting blood glucose measurements were done using standard protocols. The respondents’ CVD risk was assessed using WHO prediction chart. Data were analyzed using IBM SPSS version 25; bivariate analysis was done using Chi-square and binary logistic regression was used to identify the predictors of 10-year risk for CVDs at 5% level of significance.
Results
The mean age of respondents was 46.0 + 6.7 years. The proportion of respondents with good knowledge of risk factors was 57.7%. The prevalence of CVD risk factors were as follows: systolic hypertension (29.6%), visceral obesity (35.8%), diabetes mellitus (18.8%), smoking (5.8%), elevated total cholesterol (55.4%) and physical inactivity (84.6%). The proportion of respondents with low, moderate and high risk of developing CVDs within 10 years was 76.9, 8.5 and 14.6% respectively. Respondents with age ≥ 40 years (aOR = 2.6, 95% CI = 1.3–8.5), management cadre (aOR = 3.8, 95% CI = 1.6–9.6), obesity (aOR = 4.8, 95% CI = 1.2–120), abnormal waist circumference (aOR = 2.8, 95% CI = 1.3–5.2) and physical inactivity (aOR = 2.4, 95% CI = 1.2–4.7) were associated with the higher likelihood of developing CVDs.
Conclusion
About one-sixth of the respondents had high risk of developing CVDs within the next 10 years and it is likely that it will reduce the productivity of the State. Lifestyle modification and early detection of risk factors through regular screening programmes for those with high CVD risk is therefore recommended.
Similar content being viewed by others


Background
Cardiovascular diseases (CVDs) are known as a group of heart and blood vessel-related disorders [1]. Globally, CVDs have continued to ravage the existence of human race and equally threatened the productive sector of many countries through premature deaths of their workforce [2]. It remains a disease of public health importance due to the attendant high morbidity and mortality [3]. Worldwide, CVDs are the number one cause of death as more people die annually from it than any other causes [3, 4]. In 2015, about 17 million premature deaths occur in global south due to non-communicable disease (NCD), of which 37% were caused by CVDs. In 2016, an estimated 17.9 million people died from CVDs, representing 31% of all global deaths [3, 4]. More than three-quarters of the global deaths from CVDs occur in developing nations [5].
Hitherto, the health system in the developed world was greatly challenged with these high burdens of CVDs and its complications, but in recent times, there was a reversal of this ugly trend due to medical advances, improved healthcare delivery and good health-seeking behaviours [6]. However, in the global south, there is a significant rise in the incidence of CVDs resulting from epidemiological transition, increased urbanization and poor knowledge of risk factors for CVDs [7, 8]. This has resulted in an increased mortalities among the working populations [9].
The recent rise in CVDs in developing countries, including Nigeria has almost reached epidemic proportion [10] and this has led to a renewed effort to reinforce the use of affordable preventive strategies to stem this tide. For example, CVDs accounted for estimated 12% of all deaths in Nigeria [11] and a large percentage of medical admissions in a teaching hospital in south western part of Nigeria were due to CVDs [12]. Consequent upon this, WHO has identified very cost-effective interventions that are implementable even in low-resource settings for prevention and control of CVDs [5]. More importantly, these interventions need to be targeted at those with high total cardiovascular risk or those with single risk factor levels above traditional thresholds such as hypertension and hypercholesterolemia.
To determine the level of CVD risk in the individuals, the strategy involves the use of CVD risk calculators, such as the World Health Organization/International Society of Hypertension (WHO/ISH) prediction charts [5], Framingham [13], etc. Many studies have found the usefulness of these charts in quantifying individual’s risk of developing CVDs in the next 10 years [14, 15]. Their use is important in making informed decisions about the type and course of management to be instituted, especially in the low-resource settings, where skilled manpower, such as cardiologists is in short supply [16]. This prediction chart is found to be cost-effective and assess the total cardiovascular risk through the integration of risk factors (age, sex, presence or absence of diabetes, smoking status, systolic blood pressure, total serum cholesterol). Interestingly, this tool could be handled by clinicians and other health workers to prevent cardiovascular events (especially, stroke and heart attacks) in the developing countries [17].
Developing countries are faced with a double burden of diseases, lack of awareness of CVD predictors and huge health-infrastructural deficit and consequently have shown lack of capacity to handle this growing burden of CVDs. Hence, the necessity to find a primary preventive measure that will reduce the impact of CVDs on the lives of people in the society.
Many studies in Nigeria have focused on assessing the burden of CVD risk factors but not the risk of future cardiovascular events [18, 19]. However, information on risk factors’ prevalence alone is inadequate to provide needed knowledge on the risk of future cardiovascular events. Furthermore, for implementation of cost-effective interventions to prevent CVDs, it is essential to be equipped with information on the proportion of people in low, intermediate or high cardiovascular risk strata. This stratification affords the clinicians and non-clinician health workers the opportunity of prioritizing interventions by allocating resources to those with high total cardiovascular risk. Presently, there is scarcity of data on this in Nigeria. Therefore, this study determined the pattern and factors associated with the risk of future cardiovascular events with a view to identifying patients who are asymptomatic but at high risk of developing CVDs.
Methods
Study location
The study was conducted among local government workers in selected local government areas (LGAs) in Oyo State. Oyo state is situated in the South-western part of the country. The state has a projected 2019 population of 8, 635, 793 using a growth rate of 3.4% and 2006 population figure as the baseline [20]. Oyo State is mainly inhabited by the Yoruba ethnic group who is primarily agrarian but has a predilection for living in high-density urban centres where some are traders, artisans and civil servants. The civil servants and majority of the people are involved in trading activities which are largely sedentary. In Nigeria, the ratio of a cardiologist to population is 1: 581,000 [16]. There are three tertiary health facilities in the state. There are about 60 fast food joints and restaurants (registered) while many are unregistered, four stadia and three recreational facilities.
Study design and population
This was a descriptive cross-sectional study carried out in six selected local government areas (LGAs) of Oyo State between July and September, 2017. The study population included all the civil servants working in the LGAs’ administrative headquarters (LGA secretariats) in Oyo State at the time of study. All consenting workers who had been in the service for at least one year were recruited for the study. Pregnant women, medically unfit persons with oedema, ascites or other chronic illnesses and those who could not stand straight for weight and height measurement were excluded. Also exempted from the study were the respondents with a history of CVDs.
Sample size and sampling technique
The minimum sample size was calculated using the sample size formula for estimating single proportion. Based on the previous study on hypertension in Delta State [21], a prevalence of 21.0% was used and the margin of error was set at 5%. A non-response rate of 10% was envisaged among our respondents and adjustment for this was made to arrive at a minimum sample size of 260. A multi-stage sampling technique was used. Stage one: Two LGAs were selected from each of the list of the LGAs in each of the three senatorial districts by ballot making 6 LGAs in all. Stage two: Each LGA headquarters has 8 departments and 4 departments were selected from each of the 6 selected LGAs using ballot technique. The number of civil servants interviewed was proportionately allocated to the LGAs. Stage three: The respondents were selected using systematic sampling and this was achieved with the aid of staff nominal list retrieved from the selected LGAs.
Research instruments and data collection methods
A semi-structured interviewer-administered questionnaire adapted from WHO STEPS instrument [22] was used to collect information about respondents. Other questions developed from previous local studies were added to supplement WHO STEPS questionnaire so as to reflect local context [23, 24]. Questionnaire was used to collect data on socio-demographic characteristics, knowledge of cardiovascular risk factors, behavioural risk factors and medical history among the local government workers. Anthropometric measurements were carried out for physical assessments using stadiometer (SECA 213 Height Measure, Leicester, UK) to measure height to the nearest 0.1 m, digital bathroom weighing scale (SECA Clara 803 weight Scale, GmbH & Co, Germany) for weight measurement and non-elastic tape measure (Goldfish brand) was used to measure waist and hip circumference. All measurements were carried out in line with recommended standard protocols [25].
The respondents’ blood pressure was measured with OMRON 2 digital sphygmomanometer and this was done on the left arm having had at least 10 to 15 min of rest while respondents were sitting down. The cuffs were applied evenly and closely around the bare upper arm, with the lower edge 2.5 cm above the cubital fossa. The cubital fossa was approximately at heart level. The recorded blood pressure was an average of two measurements taken 10 mins apart.
The day preceding the study, text messages were sent to the respondents to remind them to fast overnight for the fasting lipid analysis. Ten (10) mls blood samples were collected on the spot and divided into lithium heparinized and flouride oxalate bottles from participants after an overnight fasting (8-12 h). Standard infection prevention procedures were applied in collecting blood samples from participants. The samples collected were centrifuged at 5000 g for 10 min and the plasma obtained was stored at − 20 °C in cryovials until assayed. The lipid profile was estimated by enzymatic techniques with Randox Kits using Semi-autoanalyzer (Clinical Chemistry Analyzer, HA-1900 by HAWSDEY). Fasting plasma glucose was estimated by the Glucose Oxidase method using Randox Kits. Data on 10-year risk of CVDs were captured with the WHO/ISH prediction chart [26] which makes use of age, sex, smoking status, diabetes status, systolic hypertension and total cholesterol.
Nine Community Health Extension Workers (CHEWs) and nurse/midwives who were primary healthcare staff were recruited and trained to assist in data collection. They were trained for 2 days for 3 h daily by the principal investigator on questionnaire administration and blood sample collection for lipid profile analysis and blood glucose estimation. The training involved practical demonstrations on the use of the data capturing tools. Lipid profile analysis was carried out by chemical pathologists in LAUTECH Teaching Hospital, Ogbomoso, Oyo State. The instrument was pretested among workers in local government areas different from the ones used for the main study. The pretest helped to assess the appropriateness of the questions in eliciting responses from the participants. Ambiguous questions were either removed or replaced in line with study objectives.
Measurement of outcome variables
Hypertension was defined in a respondent as one with a history of hypertension diagnosed by a physician, was using anti-hypertensive drugs, or had a systolic blood pressure (SBP) ≥140 mmHg and/or a diastolic blood pressure ≥ 90 mmHg [27]. A respondent was considered to have diabetes mellitus if he or she had been previously diagnosed by a physician, was using blood sugar lowering medications, or had a fasting blood sugar measurement of > 126 mg/dL [28].
Obesity was defined as a BMI of ≥30 kg/m2. Tobacco use was categorized as ever smoked and non-smokers. The subjects who engaged in leisure-time physical activity (walking, fitness training and sports) for greater than or equal to three times per week of 30 min per occasion were classified as physically active [29]. Visceral obesity was defined as waist circumference greater than 88 cm in females and greater than 102 cm in males [30] while the Waist-hip ratio (WHR) was considered to be abnormal if it is greater than 0.85 in female and 0.90 in male [30].
The 10-year risk of fatal/nonfatal cardiovascular events was calculated using the World Health Organization/International Society of Hypertension (WHO/ISH) risk charts calibrated for use in Region of Africa, sub-region D (AFR D) [31]. Low, moderate and high CVD risks were defined as the presence of the estimated 10-year CVD risk of < 10, 10% - < 20% and ≥ 20% respectively.
Data analysis
The data were checked daily on the field and Statistical Package for Social Sciences (SPSS) version 25 (SPSS Inc., Chicago, IL, IBM Version) was used for entry and analysis. Univariate analysis of all the variables measured was first carried out. Data were presented using frequency distribution tables and charts. Association between 10-year risk for CVDs and other categorical variables was assessed using chi square. For every cell with an expected value less than 5, Fisher’s Exact Test was used to determine the statistical significance. In the multivariate analysis, stepwise model of binary logistic regression analysis was done to determine the predictors of future CVD risk. Variables imputed into the logistic model were selected based on their level of significance during bi-variate analysis. Adjusted odds ratio and 95% confidence interval were obtained to identify determinants of 10-year risk for CVDs. The primary outcome measure of the study was 10-year risk for CVDs and re-categorized into high or low risk of developing cardiovascular events within 10 years using WHO/ISH prediction chart. Re-categorization was done by merging those with moderate and high risk into high risk. Respondents’ knowledge of CVD risk factors was tested with 10 questions and total obtainable score was 10, score above or equal to mean score (6) was categorized as good knowledge. Level of significance was set at p < 0.05 for this study.
Ethical considerations
Ethical approval for the study was obtained from the Ethical Review Committee, LAUTECH Teaching Hospital, Ogbomoso (No: LTH/OGB/EC/2016/101). Permission was obtained from the Heads of Local Government Administration of the selected LGAs. Written informed consent was obtained from study participants before they could participate in the study. Participation was voluntary and confidentiality was ensured. Anonymity was ensured by using codes rather than participants’ names as identifiers. Data were stored in a computer that was only accessible to the principal investigator. Study participants detected to have had high risk of developing CVDs within the next 10 years were appropriately counseled and referred to specialists for expertise management.
Results
Socio-demographic characteristics of LGA civil servants in Oyo state
The mean age of the respondents was 46.4 ± 6.7 years. The age of the youngest and oldest respondents was 28 years and 60 years respectively. Majority 210 (80.8%) of them belonging to age 40 years and above. Nearly all 257 (98.8%) the respondents were from Yoruba ethnic group and most of them were married 228 (88.1%). Proportions of male and female were almost the same. A little less than three-quarter 186 (71.5%) of the respondents practiced Christianity. More than half 151 (58.1%) of the respondents had tertiary education while only 17 (6.5%) of them had primary education. Majority 242 (93.1%) of them had spent more than 10 years in service. Majority 242 (93.1%) of the respondents received monthly income of greater than minimum wage (N18, 000) Table 1.
Distribution of risk factors among LGA civil servants in Oyo state
The prevalence of abnormal waist circumference, ever smoked tobacco and alcohol consumption was 93 (35.8%), 15 (5.8%) and 68 (26.2%) respectively while 220 (84.6%) and 64 (24.6%) were recorded for physical inactivity and obesity respectively. Systolic hypertension, hypercholesterolaemia, low HDLc, high LDLc, diabetes and poor knowledge of CVD risk factors were found with prevalence of 77 (29.6%), 144 (55.4%), 183 (70.4%), 59 (22.7%), 49 (18.8%) and 110 (42.3%) respectively Table 2.
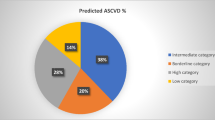
Stratification of CVD risk among local government civil servants
The proportion of respondents with low risk of developing cardiovascular event was 200 (76.9%) while the proportion of those with moderate and high risk of developing cardiovascular events was 22 (8.5%) and 38 (14.6%) respectively Fig. 1

Stratification of CVD risk among local government civil servants in Oyo State
Association between socio-demographic variables and 10-year risk for CVDs among the respondents
The proportion of those with high risk of developing CVDs increased with age and was significantly higher 55 (25.5%) among respondents with age 40 years and above (p = 0.043). The proportion 40 (66.7%) was also significantly higher among respondents who belonged to the junior cadre (p = 0.003). Those respondents with higher service years (> 10 years) were found to have greater proportion 56 (93.3%) of respondents with CVD risk (p = 0.003). There was a significantly higher proportion 58 (23.9%) of high risk of CVDs among the respondents with secondary and tertiary education (p = 0.033) Table 3.
Association between risk factors and 10-year risk for CVDs among the respondents
The proportion of those with high risk of developing CVDs was significantly higher 31 (31.9%) among respondents with abnormal abdominal circumference (p = 0.014) while it was also higher 51 (85.0%) among the respondents who added salt to the already cooked food (p = 0.049). Higher proportions of 53 (88.3%) and 21 (32.8%) of respondents with high risk of developing CVDs were prevalent among those who were physically inactive (p = 0.023) and obese (p = 0.033) respectively Table 4.
Predictors of 10-year risk for CVD among the LGA civil servants
The binary logistic regression analysis shows that the age ≥ 40 years was associated with the higher likelihood (2.6) of developing CVD within the next 10 years compared with age < 40 years. (aOR; 2.6, CI; 1.34–8.54). Also the respondents in the management cadre were associated with the higher likelihood (3.8) of developing CVD within the next 10 years compared with those in the junior cadre categories (aOR; 3.8, CI; 1.52–9.64). The respondents with general obesity was associated with the higher likelihood (5.0) of developing CVD within the next 10 years compared with underweight respondents (aOR; 4.79, CI; 1.18–120.10) while those with central obesity was associated with the higher likelihood (2.8) of developing CVD within the next 10 years compared with those without central obesity (aOR; 2.8, CI; 1.32–5.20). Physical inactivity was associated with the higher likelihood (2.4) of developing CVD within the next 10 years compared with those who were physically active Table 5.
Discussion
Stratifying populations into low, moderate and high cardiovascular risk using WHO/ISH prediction charts is one of the important ways of ensuring the allocation of scarce resources to reduce the magnitude of cardiovascular outcome, especially in the groups with high cardiovascular risk. This study determined the proportion of local government workers in different categories of risk levels that would develop CVDs in the next 10 years using the WHO/ISH scoring system [31]. Our study revealed that more than two-thirds of local government workers belong to a low risk category and this was consistent with 72.6% [32] reported in United States. The high prevalence of low cardiovascular risk in this study could be due to good knowledge on risk factors. However, this was lower than 83.0% [33], 86.4% [34] and 92.6% [35] documented in India, Nepal and Saudi Arabia respectively. The low prevalence recorded in this study could probably be attributed to different study populations, especially in age distribution. In our study, the mean age was 46.4 (± 6.7) years while the mean ages in the above studies were 54.2 (±11.1) years and 53.5 (±10.1) years.
Our study also revealed 8.5% of respondents were in moderate risk of developing CVDs in the next 10 years and this was in agreement with 7.9% reported in Angola [36]. However, it was lower than 15.5 and 31.1% documented in U.S [32] and a rural community in Nigeria [37] respectively. This finding signifies the proportion of local government workers who need individualized lifestyle interventions and perhaps drug treatment considerations.
The proportion of respondents with high risk of coming down with CVDs was 14.6% and this is suggestive of those in critical need of pharmacological interventions. This proportion needs not only intensified lifestyle modification but drugs inclusion is a must in order to avert the impending CVDs. With respect to other similar studies, the prevalence of high risk of developing CVDs found in this study was in agreement with that of India (13.2%) [38] and the United States (15.5%) [39]. However, it was higher than those of rural India (10.2%) [15], Sri Lanka (2.2%) [40] and Cambodia (10.4%) [41] and lower than the Mongolian (33.3%) and Malaysian (20.8%) [41] studies. The implication of this finding is that more people will be in need of drug treatment which is probably outside their financial capacities; hence, there is an urgent need to put primary preventive measures on ground to reverse this situation.
The higher proportion recorded in our study could result from population of civil servants who are viewed as susceptible to CVD risk factors [42]. This could also result from high prevalence of systolic hypertension, total serum cholesterol, obesity and physical inactivity recorded among the study participants. However, the lower prevalence reported in our study compared with Mongolian and Malaysian studies could result from older population and a higher life expectancy at birth [43]. This is corroborated by the findings in Indonesia that increasing life expectancy and urbanization are major determinants of CVDs in developing countries [7].
Furthermore, the prevalence of high cardiovascular risk is equally lower than what was reported by Emerole in the tertiary institutions in Nigeria [44]. This lower prevalence could probably result from low socio-economic status of the respondents compared with what obtains in the university settings, since poverty has been found to be associated with a higher risk of heart-related mortalities [45].
Age was found to be one of the determinants of 10-year risk of CVDs. Respondents with age greater than 40 years were about 3 times associated with the higher likelihood of developing CVD compared with those in the age 40 years and below. This could be reasoned from the fact that those above 40 years of age belonged to the high income earners and they were mainly from the management cadre and this has been found to be associated with increased incidence of CVD risk factors [42, 46]. This is corroborated by a study in Nigeria where a higher risk of CVDs among high income earners was documented [23]. Arising from this finding, those respondents in this age category should be prioritized for screening of CVD risk factors with possible pharmacological interventions.
It was also reported from our study that respondents from the management cadre were about 4 times associated with the higher likelihood of developing CVD within the next 10 years compared with their junior cadre staff counterparts and this was consistent with a study in Sri Lanka where a respondent’s grade was found to be a stronger predictor of his subsequent cardiovascular events [47]. Evidence from our study in support of this was the higher significant difference in obesity between management (53.2%) and junior (22.4%) cadre staff.
In addition, our study also reported obesity as a determinant of CVDs as it confers about 5 times likelihood of developing CVDs compared with non-obese respondents. This is not surprising because obesity has been reported to be strongly related to major cardiovascular risk factors such as raised blood pressure, glucose intolerance, type 2 diabetes and dyslipidaemias [28]. The increased obesity noticed in this study, may generally reflect the nutritional transition being reported in developing countries, where lifestyle changes in the direction of high energy diet and sedentary habits are taking an upward turn [48]. This may be the probable reason why the prevalence rate of obesity that was reported in this study almost doubles the findings by Amole [24] in the same Oyo State 6 years ago. However, it may just be a reflection of the socio-economic status of the different study areas [23]. If higher risk of CVDs is to be reduced, therefore education of people on the risk factors for obesity and weight reduction through non-pharmacological means will be imperative.
Respondents with abnormal waist circumference were about 3 times more likely to come down with CVDs than those with normal values. Arising from this fact, it is recommended that waist circumference should be a routine measure in clinical practice to characterize health risk and of equal importance, to follow the success of strategies designed to reduce obesity and related co-morbid conditions. Those who were physically inactive were 2.4 times associated with the higher likelihood of developing CVD compared with respondents who were active. The physical inactivity amplifies the effects of other risk factors like hypertension, triglycerides, diabetes and obesity which in turns increases the risk of CVD [49]. This is in agreement with a cross-sectional study of middle-aged premenopausal women where physical activity was seen to significantly lower blood pressure, cholesterol and triglycerides [50]. As it is important for physical exercise to be encouraged by the government, so also is the need for employers to allow some time-out for physical activities among those whose work remains largely sedentary. This will help to prevent the rising prevalence of physical inactivity noticed in this study.
Study limitation
Part of the information obtained for the study was through a questionnaire and as such the study was limited by the information supplied by the respondents as some of them found it difficult to reveal some of their attributes. However, the importance and benefits of giving correct information was explained to them in order to reduce the effects of not supplying correct information.
Conclusion
The use of the WHO/ISH prediction charts in stratifying local government civil servants into low (< 10%), moderate (10–20%) and high (> 20%) level of cardiovascular risk is one of the crucial steps to identify and reduce the population eligible for drug intervention with a view to reducing the magnitude of cardiovascular events. Among the civil servants in Oyo State, about one-sixth (14.6%) of them will probably require more than lifestyle modification in the prevention and control of future cardiovascular events. Lifestyle modification and early detection of risk factors through awareness and regular screening programmes for those with high CVD risk is therefore recommended.
Availability of data and materials
Upon request, we can offer onsite access to external researchers to the data analyzed at the department of Community Medicine, LAUTECH Teaching Hospital, Ogbomoso, Nigeria. To do so, Dr. Olaniyan Akintunde Babatunde should be contacted.
Abbreviations
- LGAs:
-
Local government areas
- CVDs:
-
Cardiovascular diseases
- CHEWs:
-
Community health extension workers
- LAUTECH:
-
Ladoke Akintola University of technology
- LTH:
-
LAUTECH teaching hospital
- WHO:
-
World Health Organization
- ISH:
-
International Society of Hypertension
- LDLc:
-
Low density lipoprotein cholesterol
- HDLc:
-
High density lipoprotein cholesterol
- BMI:
-
Body mass index
References
World Health Organisation. Global atlas on cardiovascular disease prevention and control. 2011. whqlibdoc.who.int/publications/2011/9789241564373_eng.pdf.
Thomas AG, Michael JG. Global Burden of cardiovascular Disease: Braunwald’s Heart Disease; A textbook of Cardiovascular Medicine. 9th ed. Philadelphia: Elsevier’s Health Sciences Right Department; 2011. p. 1–20.
Department of Chronic Diseases and Health Promotion, World Health Organization. Preventing chronic diseases: a vital investment. Geneva: World Health Organization; 2005.
The world health report 2002: reducing risks, promoting healthy life. Geneva: World Health Organization; 2002.
World Health Organization. Prevention of cardiovascular disease: guidelines for assessment and management of total cardiovascular risk. Geneva: WHO; 2007.
World Health Organization (WHO). Cardiovascular diseases - Fact sheet N°317 [internet]. 2013. Available from: http://www.who.int/mediacentre/factsheets/fs317/en/.
Maharani A, Sujarwoto, Praveen D, Oceandy D, Tampubolon G, Patel A. Cardiovascular disease risk factor prevalence and estimated 10-year cardiovascular risk scores in Indonesia: The SMARThealth Extend study. PLoS One. 2019;14(4):e0215219.
National Health Survey of Pakistan 1990–1994. Pakistan Medical Research Council, 1998.
Gaziano TA. Reducing the growing burden of cardiovascular disease in the developing world. Health Aff (Millwood). 2007;26(1):13–24.
Murray CJL, Lopez AD. The global burden disease. A comprehensive assessment of mortality and disability from disease, injuries, and risk factors in 1990 and projected to 2020. Cambridge: Harvard University Press; 1996.
Ala A, Timothy A, Melanie C, Leanne R. Noncommunicable diseases country profiles 2011. WHO. 2011:1–207. https://apps.who.int/iris/bitstream/handle/10665/44704/9789241502283_eng.pdf?sequence=1.
Okunola OO, Akintunde AA, Akinwusi PO. Some emerging issues in medical admission pattern in the tropics. Niger J Clin Pract. 2012;15(1):51–4.
D’Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, Kannel WB. General cardiovascular risk profile for use in primary care: the Framingham heart study. Circulation. 2008;117(6):743–53.
Mendis S, Lindholmb LH, Andersonc SG, Alwana A, Kojud R, Onwuberee BJC, Kayanif AM, Abeysingheg N, Duneash A, Tabagarii S, Fanj W, Sarraf-Zadegank N, Nordeta P, Whitworth J, Heagerty A. Total cardiovascular risk approach to improve efficiency of cardio. J Clin Epedemiol. 2011;64(12):1451–62.
Ghorpade AG, Shrivastava SR, Kar SS, Sarkar S, Majgi SM, Roy G. Estimation of the cardiovascular risk using World Health Organization/International Society of Hypertension (WHO/ISH) risk prediction charts in a rural population of South India. Int J Health. 2015;4(8):531–6.
Sliwa K, Zühlke L, Kleinloog R, Doubell A, Ebrahim I, Essop MF, et al. Cardiology-cardiothoracic subspeciality training in South Africa: A position paper of the South Africa Heart Association. Cardiovasc J Afr. 2016;27(3):188–93.
Conroy RM, Pyorala K, Fitzgerald AP, Sans S, Menotti A, De Backer G, De Bacquer D, Ducimetière P, Jousilahti P, Keil U, Njølstad I, Oganov RG, Thomsen T, Tunstall-Pedoe H, et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: the S. Eur Heart J. 2003;24(11):987–1003.
Sani MU, Wahab KW, Yusuf BO, Gbadamosi M, Johnson OV, Gbadamosi A. Modifiable cardiovascular risk factors among apparently healthy adult Nigerian population-a cross sectional study. BMC Res Notes. 2010;3:11.
Amole IO, OlaOlorun AD, Odeigah LO, Adesina SA. The prevalence of abdominal obesity and hypertension amongst adults in Ogbomoso, Nigeria. Afr J Prim Heal Care Fam Med. 2011;3(1):1–5 Available from: www.phcfm.org/index.php/phcfm/article/view/188. Accessed 12 Oct 2014.
Federal Republic of Nigeria Official Gazette. Legal Notice on Publication of 2006 Census Final Results. 2009;96(2):B1–42.
Ibekwe R. Modifiable risk factors of hypertension and socio-demographic profile in Oghara, Delta state; prevalence and correlates. Ann Med Health Sci Res. 2015;5(1):71–7.
STEPS Manual for chronic diseases and health promotion. [http://www.who.int/chp/steps/manual/en/]. Accessed 22 Feb 2019.
Karaye KM, Okeahialam BN, Wali SS. Cardiovascular topics impact of income on the profile of cardiovascular risk factors among hypertensives in a Nigerian tertiary health Centre : a cross-sectional study. Cardiovasc J Afr. 2009;20(4):251–5.
Amole IO, Olaolorun AD, Owolabi AO. Prevalence of obesity and hypertension among adults in Ogbomoso, Nigeria. Internet J Med Update. 2011;6(2):9–14.
International Society for the Advancement of Kinanthropometry. International Standards for anthropometric Assessment; 2001. p. 53–5.
WHO/ISH Risk prediction charts for 14 WHO epidemiological sub-regions [internet]. 2007. [cited 2017 Nov 19]. Available from: http://ish-world.com/downloads/activities/colour_charts_24_Aug_07.pdf.
Hendriks ME, Wit FW, Roos MT, Brewster LM, Akande TM, Ingrid H. Hypertension in sub-Saharan Africa: cross-sectional surveys in four rural and urban communities. PLoS One. 2012;7(3):e32638.
Mendis S, Puska P. Global Atlas on Cardiovascular Disease Prevention and Control. Geneva: World Health Organization (in collaboration with the World Heart Federation and World Stroke Organization); 2011.
Physical Activity and Health. A report of the Surgeon General. Washington DC: US department of health and human services; 2008. (cited 2008 Oct 17); Available from:http://www.surgeongeneral.gov/library/disabilities/calltoaction/whatitmeanstoy.
World Health Organization. Definition, Diagnosis, and Classification of Diabetes Mellitus and its Complications: Report of a WHO Consultation. Part I: Diagnosis and Classification of Diabetes Mellitus. Geneva: World Health Organization; 1999. Accessed on 26 January 2018.
World Health Organization. Prevention of Cardiovascular Disease, Pocket Guidelines for Assessment and Management of Cardiovascular Risk. Geneva; 2007. http://www.who.int/cardiovascular_diseases/guidelines/PocketGL.ENGLISH.AFR-D-E.rev1.pdf.
Ford Earl S, Giles WH, Mokdad A. The distribution of 10-year risk for coronary heart disease among U.S. adults: findings from the National Health and nutrition examination survey III. J Am Coll Cardiol. 2004;43(10):1791–6.
Ghorpade AG, Shrivastava SR, Kar SS, Sarkar S. Estimation of the cardiovascular risk using World Health Organization/International Society of Hypertension (WHO/ISH) risk prediction charts in a rural population of South India. Kerman Univ Med Sci. 2015;4(8):531–6 Available from: https://doi.org/10.15171/ijhpm.2015.88.
Khanal MK, Ahmed MSA, Moniruzzaman M, Banik PC, Dhungana RR, Bhandari P, Devkota S, Shayami A. Total cardiovascular risk for next 10 years among rural population of Nepal using WHO/ISH risk prediction chart. BMC Res Notes. 2017;10(1):120 Available from: http://bmcresnotes.biomedcentral.com/articles/10.1186/s13104-017-2436-9.
Soofi MA, Youssef MA. Prediction of 10-year risk of hard coronary events among Saudi adults based on prevalence of heart disease risk factors. J Saudi Hear Assoc. 2014;27(3):152–9 Available from: https://doi.org/10.1016/j.jsha.2015.03.003.
Pedro MJ, Brito M, Barros H. Cardiovascular Risk Assessment in Angolan Adults: A Descriptive Analysis from CardioBengo, a Community-Based Survey. Int J Hypertens. 2018;2018:6.
Ogunmola JO, Olaifa OA, Akintomide AO. Assessment of cardiovascular risk in a Nigerian rural community as a means of primary prevention evaluation strategy using Framingham risk calculator. IOSR J Dent Med Sci. 2013;7(3):45–9.
Geldsetzer P, Manne-Goehler J, Theilmann M, Davies JI, Awasthi A, Danaei G, Gaziano TA, Vollmer S, Jaacks LM, Barnighausen T, Atun R. Geographic and sociodemographic variation of cardiovascular disease risk in India: A cross-sectional study of 797,540 ad. PLoS Med. 2018;15(6):e1002581 Available from: https://doi.org/10.1371/journal.pmed.1002581. eCollection 2018 Jun.
Ford ES, Giles WH, Mokdad A. The distribution of 10-year risk for coronary heart disease among US adults findings from the National Health and nutrition examination survey III. Coron Artery Dis. 2004;43(10):6–11.
Mendis S, Lindholm LH, Anderson SG, Alwan A, Koju R, Onwubere BJ, Kayani AM, Abeysinghe N, Duneas ATS. Total cardiovascular risk approach to improve efficiency of cardiovascular prevention in resource constrain settings. J Clin Epidemiol. 2011;64(12):1451–62.
Otgontuya D, Oum S, Buckley BS, Bonita R. Assessment of total cardiovascular risk using WHO/ISH risk prediction charts in three low and middle income countries in Asia. BMC Public Health. 2013;13(1):539 https://doi.org/10.1186/1471-2458-13-539.
Gyntelberg F, Suadicani P, Jensen G, Schnohr P, Netterstrom B, Kristensen TS. Job strain and cardiovascular risk factors among members of the Danish parliament. Occup Med (Lond). 1998;48(1):31–6.
World Bank Country Data. http://databank.worldbank.org/data/views/reports/tableview.aspx. Accessed 12 May 2018.
Emerole CO, Aguwa EN, Onwasigwe CN, Nwakoby BAN. Cardiac risk indices of staff of Federal University of Technology Owerri, Imo state, Nigeria. Tanzan Health Res Bull. 2007;9(2):132–5.
Mensah GA, Mokdad AH, Ford ES, Greenlund KJ, Croft JB. State of disparities in cardiovascular health in the United States. Circulation. 2005;111(10):1233–41.
Ugwuja EI, Ogbonna NC, Nwibo A, Onimawo IA. Overweight and obesity, lipid profile and Atherogenic indices among civil servants in Abakaliki, south eastern Nigeria. Ann Med Health Sci Res. 2013;3(1):13–8.
Herath MM, Thilak Priyantha W, Umesha D. Cardiovascular risk assessment in type 2 diabetes mellitus : comparison of the World Health Organization / International Society of Hypertension risk prediction charts versus UK Prospective Diabetes. Vascular. 2015;11:583–9.
Dominguez LJ, Galioto A, Ferlisi A. Aging, lifestyle modifications and cardiovascular disease in developing countries. J Nutr Heal Aging. 2006;10:143–9.
Kokkinos P. Physical activity and cardiovascular disease prevention: current recommendations. Angiology. 2008;59(2):26S–9S.
Owens JF, Matthews KA, Wing RR, Kuller LH. Physical activity and cardiovascular risk: a cross-sectional study of middle-aged premenopausal women. Prev Med. 1990;19(2):147–57.
Acknowledgements
The authors appreciate the Head of Local Government Administration and the Local Government Staff that participated in the study for their cooperation.
Funding
No financial support was received for this research.
Author information
Authors and Affiliations
Contributions
OAB conceptualized the study, JOB and OS contributed to the design, JOA supervised laboratory analysis, OAB drafted the initial manuscript, OAB, AAA, AB, JOB, SOO, CDU and JOA contributed to the analysis, interpretation of the results and made substantial revision to the initial draft. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Approval for the study was obtained from the Ethical Review Committee, LAUTECH Teaching Hospital, Ogbomoso, Oyo State (No: LTH/OGB/EC/2016/101). All participants were informed about the study and confidentiality protocols. Written Informed consent was obtained from all the participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Babatunde, O.A., Olarewaju, S.O., Adeomi, A.A. et al. 10-year risk for cardiovascular diseases using WHO prediction chart: findings from the civil servants in South-western Nigeria. BMC Cardiovasc Disord 20, 154 (2020). https://doi.org/10.1186/s12872-020-01438-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-020-01438-9