
Abstract
Purpose of Review
To describe robotic-assisted peritoneal vaginoplasty in the genital gender affirming surgical setting and demonstrate existing surgical outcomes.
Recent Findings
Robotic peritoneal vaginoplasty is similar to a posterior approach to a robotic-assisted laparoscopic prostatectomy and can be done utilizing both multi-port and single port robotic platforms. Neovaginal canal depths and widths of 14 ± 0.7 cm by 3.6 ± 0.2 cm respectively can be obtained. Peritoneal flaps can also augment neovaginal depth by approximately 5 cm beyond the length of a skin graft or flap, proving advantageous in cases of genital hypoplasia or canal depth loss requiring revision. Patients typically report high sexual satisfaction following vaginoplasty.
Summary
The robotic peritoneal vaginoplasty as a genital gender affirming surgery offers additional neovaginal depth, with reported low complication rates, acceptable cosmesis, and satisfactory sexual function. Ongoing research in alternative grafts and revision remain to be studied.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Robotic peritoneal vaginoplasty for gender affirming genital surgery has been adapted from a series of surgeries well-known to gynecologic surgeons adapted from the surgical management of congenital vaginal absence, most notably for those affected by Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome [1]. The McIndoe-Reed vaginoplasty, which involved the creation of a neovaginal space between the rectum and bladder, followed by the insertion of a skin graft [1,2,3] often resulted in complications such as graft contraction, stenosis, and donor site morbidity, which impacted the overall satisfaction and sexual function of the patients [3]. Surgical alternatives stemmed from limited anatomic results, which included pull-through vaginoplasty, Singaporean flap vaginoplasty, and Lee's vaginoplasty were developed to address these shortcomings [1]. These methods varied in complexity and outcomes, with each offering certain advantages over the McIndoe-Reed technique.
Despite these advancements, a significant breakthrough came with the introduction of the Davydov procedure. This technique marked a departure from the reliance on skin grafts or external materials by utilizing the patient's own peritoneum to line the newly created vaginal canal [1,2,3]. The Davydov technique begins with the dissection of the rectovesical space, followed by the creation of a neovaginal cavity through careful sharp and blunt dissection. The peritoneum is then mobilized, either through laparoscopic, robotic, or open techniques, and pulled down to the vaginal introitus, where it is attached and secured [2, 3]. The Davydov procedure offered several advantages, including reduced donor site morbidity, minimized risk of graft rejection, and improved outcomes in terms of anatomical correction and sexual functionality. Its minimally invasive nature, combined with the use of the body's natural tissues, made it a preferred option for many surgeons and patients alike [4]. The evolution from initial vaginoplasty techniques to the Davydov procedure represents a significant advancement in the treatment of MRKH syndrome and underscores a shift towards more anatomically and functionally satisfactory outcomes, which paved the way for its adaptation to robotic-assisted peritoneal vaginoplasty in the genital gender affirming surgical world.
Davydov Procedure: Comparative Techniques and Modifications
Over time, the modified McIndoe technique has largely been replaced by the Davydov procedure for various reasons [2, 3]:
-
Anatomical Results: The Davydov technique generally results in a neovagina that is more anatomically congruent with natural vaginal dimensions, contributing to improved sexual function.
-
Sexual Performance and Satisfaction: Patients undergoing the Davydov procedure reported higher levels of sexual satisfaction, attributed to the natural feel and function of the neovagina created using the patient's peritoneum.
-
Patient Recovery: Although the laparoscopic Davydov group experienced longer operative times, the outcomes in terms of mold retention, return of bowel activity, and overall recovery were found to be satisfactory.
Of note, operating times are generally longer for the laparoscopic Davydov procedure in comparison to laparoscopic McIndoe technique due to the meticulous nature of the peritoneal mobilization and attachment [3]. However, this extended operative time is justified by the outcomes, which include successful mold retention, indicating the neovagina's stability and durability, and efficient patient recovery, allowing for a quicker return to normal activities.
Transition to Robotic Peritoneal Vaginoplasty
The transition from traditional surgical techniques to robotic-assisted procedures is a pivotal development in vaginoplasty. This shift leverages the latest in medical technology to address the limitations of previous methods, offering a range of benefits that enhance both the surgical process and patient outcomes [6]. The adoption of robotic technology in peritoneal vaginoplasty offers several key benefits over traditional laparoscopic and open techniques:
-
Enhanced Precision: The robotic system's superior visualization and instrument control enable meticulous dissection and accurate placement of sutures, reducing the risk of injury to surrounding tissues.
-
Reduced Operative Times: Although the setup for robotic surgery may initially extend operative times, the efficiency gained through improved dexterity and precision can lead to shorter overall surgery durations as surgeons gain experience.
-
Quicker Recoveries: The minimally invasive nature of robotic-assisted surgery results in smaller incisions, less postoperative pain, reduced risk of infection, and faster recovery times, allowing patients to resume normal activities more quickly as compared to open surgery.
Robotic Peritoneal Vaginoplasty: A technical description
Robotic peritoneal vaginoplasty has been described with both the multi-port and single-port DaVinci robotic platforms. Prior to peritoneal vaginoplasty, prophylactic antibiotics are commonly administered. Common protocols include piperacillin-tazobactam, vancomycin, cefepime, and/or metronidazole given at the time of induction and maintained for 24–48 h post operatively. Many preoperative protocols included providing prophylactic heparin or enoxaparin. Surgical sterile preparation is done from the xiphoid to the proximal thighs to facilitate both abdominal and perineal approach. The patient is positioned in dorsal lithotomy and secured to the operating table for positioning in 45-degree steep Trendelenburg. There are concurrent perineal and robotic surgical teams to begin the penile inversion technique and the abdominal approach for peritoneal flap creation, respectively.
The purpose of the peritoneal approach is to anastomose the penile inversion skin flap to allow for greater depth. Robotic peritoneal vaginoplasty can also be performed in the revision setting after primary penile inversion vaginoplasty [5••, 7•].
The robotic approach begins with gaining intrabdominal access to create peritoneal flaps. Any bowel adhesions are released laterally from the pelvic sidewalls to expose the rectovesical space. The peritoneal flaps are dissected from the pelvic side walls to the posterior surface of the bladder and the pararectal fossa [5••]. A horizontal incision is made at the level of rectovesical junction over the seminal vesicles, similar to a posterior approach to a robotic-assisted laparoscopic prostatectomy. The dissection is widened beneath the vas deferens bilaterally [6]. Care must be taken from this approach to avoid ureteral and vascular pedicle injuries when creating peritoneal flaps. If the prostatic pedicle is injured in this dissection, suture ligation is the preferred hemostatic approach. Both the posterior and anterior peritoneum are dissected, ensuring more of the posterior peritoneum is spared.
The peritoneal dissection is being done simultaneously with the perineal dissection. Penile inversion vaginoplasty has been described in detail but involves a separate team performing the dissection between the rectum and prostate/bladder plane to develop the distal neovaginal canal. This is initiated by creating a rhomboid perineal flap between the ischial tuberosities and the perineal-scrotal junction. The flap is elevated to the level of the bulbar urethra. The perineal dissection continues laterally and posteriorly to achieve adequate depth and width. The scrotal skin previously removed is thinned to create a full thickness skin graft to bridge introitus to peritoneum. The vaginal canal dissection is carried posteriorly to Denonvilliers’ (rectoprostatic) fascia. The neovaginal canal depth and width can be limited by narrow pelvic dimensions or difficulty in dissecting the vaginal space [8•].
The peritoneal dissection is dependent on the dimensions achieved in the neovaginal canal and the amount of tissue available to line the neovagina. Ideally, a 12 cm by 12 cm anterior peritoneal flap from the posterior aspect of the bladder is raised with medial umbilical ligaments as lateral borders. The extent of the posterior peritoneal flap includes the rectum, medial aspect of the ureters, and the sacral promontory. Other reports have been able to safely augment neovaginal canal with 6 cm by 8 cm peritoneal flaps from the anterior and posterior aspects to meet in the midline and form the neovaginal apex [9]. Additional peritoneal flap harvest is performed to ensure tension free anastomosis to avoid peritoneal flap devascularization and dehiscence. If there is limited mobility of the peritoneal flaps, then the penoscrotal tube is lengthened with potential additional skin grafts to avoid an anastomosis on tension [5••, 7•].
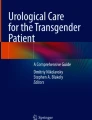
A window is developed between the perineal and pelvic dissection planes. If there is tension between the peritoneal flap and the neovagina, lateral incisions can be made along the peritoneal incisions to facilitate greater length. These flaps are then sutured anteriorly and posteriorly to the penile/scrotal skin or tubularized full thickness skin grafts that create the neovaginal canal. The posterior flap is sutured to the inferior ventral penoscrotal skin and the anterior flap is sutured to the dorsal aspect. The neovaginal apex is created using a purse string suture is performed with 2–0 or 3–0 V-lock suture in purse string fashion from the peritoneum to the skin flaps or grafts. The anterior, posterior and lateral peritoneal defects are closed with running 2–0 or 3–0 V-lock suture (Fig. 1) [5••, 7•].

Peritoneal flaps sutured using running locking V-lock suture to create the vaginal apex and the anatomic relation to the neighboring bladder, ureters and rectum
A modified single pedicled robotic peritoneal flap to augment the neovaginal canal performed with penile inversion vaginoplasty is also described as an alternative to anterior and posterior peritoneal flaps harvest. This flap is harvested only from the posterior bladder surface. This peritoneal reflection is incised and dissected to reach the neovaginal apex. The flap is reflected and sutured circumferentially to the neovaginal apex. The sides are adapted to the cul de sac posteriorly. For a single pedicled flap, a wider base must be harvested. Care must be taken to avoid suturing the superior side of the neovaginal canal which is pushed into the abdominal cavity through perineal access to avoid compromising the anastomosis and potential depth of the canal [10]. Otherwise, the remaining steps are similar for robotic peritoneal vaginoplasty.
There have also been descriptions utilizing tubularized urachus-peritoneal hinge flaps in the setting of revision vaginoplasty. In this method, the bladder is filled to demarcate the bladder margins. Urachus is thought to be more durable than only peritoneum as it has more fibrous vascularized tissue. The free end of the anterior flap by the bladder is dissected and the free end is flipped posteriorly and sutured to the posterior edge of the open canal remnant, creating a peritoneal pouch. The lateral edges of the pouch are sutured together. The anterior edge of the canal remnant is also sutured to create a watertight anastomosis. This approach is limited to patients who have at least 7 cm of primary or revision neovaginal canal. This is an alternative in the setting of limited ability to harvest the posterior peritoneal flap and to avoid potential intrabdominal rectal injury [11].
In patients who have undergone primary penile inversion vaginoplasty or vulvoplasty without canal creation, revision for insufficient neovaginal canal, neovaginal stenosis or desire for neovaginal canal can be necessary. The median time to revision for creation or revision of a neovaginal canal was 35 months. Peritoneal vaginoplasty in this setting can also provide additional depth with minimal donor site morbidity. This technique can be performed both as a primary approach to vaginoplasty and as a technique to be used in patients undergoing revision surgery [12].
There are variations in wound dressing approach following incisional closure. Some authors have used: sulfamylon/mafenide acetate and lubricant over kerlix or similar packing placed inside the neovaginal canal, a vaginal packing with mupirocin and bacitracin, or silvadene with lubricant placed prior to closure of the neovaginal apex from the abdomen with a negative pressure wound vacuum dressing over the introitus, and a foley catheter was kept in place. Additional dressings with kerlix are placed over a dressing with elastic tape to maintain the dressing [5••, 7•, 11].
Robotic Peritoneal Flap Gender-Affirming Vaginoplasty Operative Characteristics
Inpatient Recovery
As robotic peritoneal flap vaginoplasty is becoming more widely adopted, the average surgical duration was 262 ± 35 min. Length of stay is approximately 5 days given need for postoperative bedrest [9].
Postoperative Care
The vaginal packing, foley catheter and wound dressings are both removed on postoperative day 5. Once the packing is removed, the patient is permitted to ambulate. Neovaginal dilation can begin between 6 to 14 days postoperatively [5••].
Postoperative Surgical Outcomes
The average achieved neovaginal canal depth and width were 14 ± 0.7 cm by 3.6 ± 0.2 cm respectively. Peritoneal flaps were able to augment neovaginal depth by 5 cm beyond the length of a skin graft or flap, especially in settings with limited natal skin [9]. Most patients (80–86%) report ability to achieve adequate orgasm, experience neovaginal wetness or increased wetness with sexual arousal (70%) and are able to have receptive intercourse (50%) [11, 13].
Postoperative Patient Report Outcomes
Patients report high sexual satisfaction following vaginoplasty regardless of approach. Approximately 1/3 of patients can have some sexual dysfunction related to distress with sexual function disturbance. Options for patients experiencing sexual dysfunction include pelvic floor physical therapy, sex therapy, and sex surrogacy. A majority of patients (57%) report engaging in intercourse at least once per week and 36% in intercourse twice per week. However, there is a higher likelihood of pain related to sexual activities following vaginoplasty compared to pre-operative reported pain [14].
Commonly cited complications include delayed wound healing, venous thromboembolism, need for blood transfusion, incisional hematoma, infection, urinary tract infections which can be managed with conservative medical management. More serious complications include rectoneovaginal fistula, neovaginal stenosis, and need for revision surgery. Other rare complications include urethral fistula, perianal fistula, clitoral prolapse, and neovaginal cuff necrosis. Risk of insufficient depth can lead to dyspareunia and promote persistent gender incongruence [15].
The management of postoperative complications following robotic peritoneal vaginoplasty can require additional operative intervention. In a series of 174 patients, those who experienced postoperative hematoma required a diagnostic laparoscopic exploration and drainage. Intrabdominal abscess is also managed the same way. Recurrent small bowel obstructions have resolved with bowel rest; however, incarcerated hernias especially if at the donor site of the peritoneum may require diagnostic laparoscopy and closure of the peritoneal flap site. In this series, no intraoperative complications were noted, as well as in other contemporary retrospective reviews of peri-operative complications [16, 17].
In a series of 245 patients, 35 patients had mainly external genital concerns and 10 underwent secondary surgery. Areas of concern included labial majora appearance, clitoral revision for hood necrosis and scarring, neourethral stenosis, meatal stenosis and neovaginal canal stenosis. These issues were sufficiently addressed with a secondary revision surgery [18].
Multi-Port vs Single Port Robotic Approach
In the Da Vinci multi-port robotic approach, a Veress needle can be placed 1–2 cm superior to the umbilicus to achieve pneumoperitoneum. The site of the Veress needle is used to place an 8 mm trocar and the camera is introduced to guide placement of 3 additional 8 mm robotic trocars approximately 10 cm apart. An open Hasson technique can also be used for camera port placement. A 12 mm assistant port is placed on the right side. An additional 5 mm assistant port can be placed in the right upper quadrant if necessary. This port placement mirrors robotic-assisted laparoscopic prostatectomy approach. The specific steps to mobilize peritoneal flaps remain the same as described earlier [7•].
The Da Vinci single port robotic approach offers a single 3 cm vertical incision superior to the umbilicus for peritoneal flap creation. This method can per preferred for overall cosmesis following vaginoplasty. Once vertical fasciotomy is created, the peritoneum is incised under direct vision via Hasson technique and a wound retractor is placed into the incision for attachment to the single port balloon port. Insufflation to 15 mmHg is done and a 5 mm assistant port can be placed 2 fingerbreadths above the anterior superior iliac spine under direct vision. The robot is side docked. The camera is maintained in the 12 o’clock position, with the monopolar scissors in the right hand, a bipolar forceps in the left hand and needle driver in the 6 o’clock position [5••, 7•].
A retrospective analysis was performed of 145 transgender women who underwent robotic peritoneal flap gender-affirming vaginoplasty utilizing the Da Vinci Xi Multi-Port and the Single Port systems from September 2017 to December 2019, focusing on those with at least six months of follow-up [5••]. There were 55 patients who underwent the multi-port approach versus 90 patients who underwent the single port DaVinci robot platform. The average procedure times were significantly shorter for the single port cohort (3.7 h) compared to the multi-port cohort (4.2 h). At a mean follow-up of 11.9 months, both groups achieved good vaginal depth and width, with the single port group showing a slight improvement in vaginal depth. The study also reported comparable complication rates between the two robotic systems, including transfusion, rectovaginal fistula, bowel obstruction, pelvic abscess, and vaginal stenosis. Using the single port robot system facilitates a dual-surgeon abdominal-perineal approach, effectively reducing operative time without increasing complication rates as well [5••].
Considerations for Limitations for Insufficient Canal
In patients who experience neovaginal stenosis, salvage reconstruction with peritoneal vaginoplasty allows for recovery of neovaginal depth with minimal donor site morbidity. This has been primarily used in the setting of primary penile inversion vaginoplasty [12]. In this setting of limited genital skin, despite various options, they may still be prone to complications. If feasible, peritoneal flap harvest is a viable option with acceptable cosmetic outcomes especially when utilizing the single port robotic platform.
In patients who have undergone puberty blockade or have had prior feminizing surgeries, natal skin can be limited when pursuing primary or revision surgery. Additional factors that may impact available tissue for neovaginal canal include prior circumcision, orchiectomy, obesity, trauma, inflammatory conditions, and congenital variants. Previously intestinal vaginoplasty or extragenital split thickness skin grafts were considered options in this setting to achieve an adequate depth [9]; however, skin grafts are also prone to complications such as donor site morbidity and risk of hair growth in neovaginal canal. Intestinal flaps carry risk of bowel obstruction, anastomotic leak, and diversion colitis. The estimated depth is 15 cm from pedicled bowel vaginoplasty compared to 14 cm peritoneal flap vaginoplasty but bowel vaginoplasty is vulnerable to obstruction, excessive mucus production, diversion colitis, peritonitis, fistulae, anastomotic leaks, and foul odor [8•, 19].
Introitus reconstruction with skin graft is a viable option to preserve remaining genital tissue for other critical vulvar structures. This has been applied to patients with pubertal suppression at Tanner stage 2, limiting available genital skin for reconstruction [20]. In a series of 43 patients with genital hypoplasia compared with 49 patients with adequate natal tissue, insufficient neovaginal canal depth was considered to be < 7 cm. Peritoneal vaginoplasty in this series provided a depth of 14 cm and overall allowed for greater depth compared to standard penile inversion vaginoplasty [8•].
Dermal substitutes, like AlloDerm (BioHorizons and AbbVie, Birmingham, AL), have also been assessed as an option for insufficient peritoneal flap or skin graft in a small series of transgender patients, as it has been used in MRKH syndrome, vaginal reconstruction following oncologic resection, and vaginal repair of rectovaginal fistulas in cisgendered women. Alloderm is derived from human cadaveric skin by removing the epidermal and cellular components until only the basement membrane and collagen skeleton of the extracellular matrix remain. Estimated epithelization should occur within 3 to 6 weeks. Tubularized AlloDerm has been used as an intervening segment between the remnant neovaginal lining and the peritoneal flaps if there is insufficient peritoneal flap or tissue for neovaginal canal [21]. If the apex of the neovaginal canal is stenotic, this is incised from a robotic intrabdominal approach. The peritoneal flaps, if previously not harvested, are dissected and then measured. The interval gap between the remnant canal and the peritoneal flap is assessed if a tension free anastomosis is not possible. Two pieces of extra thin AlloDerm are then tubularized around a vaginal dilator. The tubularized AlloDerm is sutured first to the remnant canal and then to the peritoneal flap from the abdominal approach. Upon revision with AlloDerm, neovaginal median depth achieved were 12 cm by 3.5 cm with an overall increase in depth and width between 9.7 cm by 0.9 cm [21]. Patients with intact vaginal canal remnant prior to revision may have improved outcomes with pelvic floor physical therapy to enhance dilation strategies and soften scar tissue if it occurs with AlloDerm. Postoperative complications related to use of AlloDerm included granulation tissue, urinary complaints, vaginal stenosis in a third of patients. Most patients were able to achieve orgasm and confirmed clitoral sensation remained intact when AlloDerm was used [21]. For patients who experience areas of excess AlloDerm placement in the neovaginal canal postoperatively, this can be trimmed in the outpatient setting without compromising the neovaginal canal.
Approaches for local grafts and flaps include utilizing remaining scrotal skin, abdominal and thigh flaps, buccal mucosal graft, pedicled groin flaps, and perineal pedicle flaps. The latter two options may be limited in the maximal soft tissue graft available [15]. Donor site morbidity is still a consideration when harvesting these grafts or flaps. In a review of scrotal, buccal, skin, and urethral flaps, there are various risks and complications. Skin grafts are considered ideal for achieving maximal neovaginal depth, especially scrotal grafts. There is some concern regarding potential graft contracture and stenosis with skin grafts. Minor complications are considered wound dehiscence, granulation tissue, and scarring. When a buccal mucosal graft is combined with a scrotal flap, the rate of prolapse is estimated at 11% compared to those without buccal mucosal graft (0–4%) [22].
Conclusions
While there are many approaches to vaginoplasty, robotic peritoneal vaginoplasty offers additional neovaginal depth, with low complication rates, acceptable cosmesis, and many patients report satisfactory sexual function. For surgeons who are facile with minimally invasive surgery and gender affirming surgery, the single port robotic peritoneal flap approach should be included in the armamentarium when planning vaginoplasty.
Data Availability
No datasets were generated or analysed during the current study.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Passos IMPE, Britto RL. Diagnosis and treatment of Müllerian malformations. Taiwan J Obstet Gynecol. 2020;59(2):183–8. https://doi.org/10.1016/j.tjog.2020.01.003. PMID: 32127135.
Deldar-Pesikhani M, Ghanbari Z, Shahrbabaki FS, Nassiri S, Raznahan M, Shokrpour M. Comparison of modified McIndoe and Davydov vaginoplasty in patients with MRKH syndrome in terms of anatomical results, sexual performance and satisfaction. J Family Med Prim Care. 2022;11(8):4614–8. https://doi.org/10.4103/jfmpc.jfmpc_1939_21. Epub 2022 Aug 30. PMID: 36352939; PMCID: PMC9638586.
Aslan K, Gurbuz TB, Orhan A, Kasapoglu I, Ozerkan K, Uncu G. Long term sexual outcomes of Mayer Rokitansky Küster Hauser Syndrome patients after Uncu-modified Davydov procedure. Facts Views Vis Obgyn. 2023;15(3):235–42. https://doi.org/10.52054/FVVO.15.3.091. PMID: 37742200; PMCID: PMC10643009.
Elyaguov J, Schardein JN, Sterling J, Nikolavsky D. Gender Affirmation Surgery, Transfeminine. Urol Clin North Am. 2022;49(3):437–51. https://doi.org/10.1016/j.ucl.2022.05.001. Epub 2022 Jun 29 PMID: 35931435.
•• Dy GW, Jun MS, Blasdel G, Bluebond-Langner R, Zhao LC. Outcomes of Gender Affirming Peritoneal Flap Vaginoplasty Using the Da Vinci Single Port Versus Xi Robotic Systems. Eur Urol. 2021;79(5):676–83. https://doi.org/10.1016/j.eururo.2020.06.040. Largest robotic cohort of peritoneal flap vaginoplasty patients with comparative outcomes demonstrating significant success, low complication profiles, and maintained vaginal depth and width up to a year following surgery.
Martens L, Tannenbaum L, Van Kuijk SMJ, Notten KJB, Kluivers KB. Laparoscopic Davydov versus laparoscopic Vecchietti neovaginoplasty in women with Mayer-Rokitansky-Küster-Hauser syndrome; a systematic review and meta-analysis. Fertil Steril. 2023;121(4):679–92. https://doi.org/10.1016/j.fertnstert.2023.12.015. Epub ahead of print. PMID: 38104886.
• Acar O, Sofer L, Dobbs RW, Greenwald DT, Halgrimson WR, Crivellaro S, Kocjancic E. Single Port and Multiport Approaches for Robotic Vaginoplasty With the Davydov Technique. Urology. 2020;138:166–73. https://doi.org/10.1016/j.urology.2019.11.043. Epub 2020 Jan 3. PMID: 31904396. An additional team validating the application of multi and single port robotic platforms, this offered further support to robotic vaginoplasty’s efficacy and safety profile.
• Blasdel G, Kloer C, Parker A, Shakir N, Zhao LC, Bluebond-Langner R. Genital Hypoplasia before Gender-Affirming Vaginoplasty: Does the Robotic Peritoneal Flap Method Create Equivalent Vaginal Canal Outcomes? Plast Reconstr Surg. 2023;151(4):867–74. https://doi.org/10.1097/PRS.0000000000010011. Epub 2022 Dec 9. PMID: 36729740. Retrospective cohort of limited genital skin patients who underwent surgical affirmation utilizing robotic peritoneal flaps to support equivalent vaginal depth and dilation outcomes.
Jacoby A, Maliha S, Granieri MA, Cohen O, Dy GW, Bluebond-Langner R, Zhao LC. Robotic davydov peritoneal flap vaginoplasty for augmentation of vaginal depth in feminizing vaginoplasty. J Urol. 2019;201(6):1171–6. https://doi.org/10.1097/JU.0000000000000107. PMID: 30707129.
Morelli G, Zucchi A, Ralph D, Perotti A, Sollazzi E, Bartoletti R. A single pedicled robotic peritoneal flap in penile inversion vaginoplasty augmentation. BJU Int. 2023;131(1):125–9. https://doi.org/10.1111/bju.15922. Epub 2022 Oct 31 PMID: 36263846.
Smith SM, Yuan N, Stelmar J, Pa-C GL, Gupta A, Kim HL, Garcia MM. An alternative option for gender-affirming revision vaginoplasty: the tubularized Rrachus-Peritoneal hinge flap. Sex Med. 2022;10(6)100572. https://doi.org/10.1016/j.esxm.2022.100572. Epub 2022 Sep 29. PMID: 36183656; PMCID: PMC9780766.
Dy GW, Blasdel G, Shakir NA, Bluebond-Langner R, Zhao LC. Robotic peritoneal flap revision of gender affirming vaginoplasty: a novel technique for treating neovaginal stenosis. Urology. 2021;154:308–14. https://doi.org/10.1016/j.urology.2021.03.024. Epub 2021 Apr 3 PMID: 33823174.
Blasdel G, Kloer C, Parker A, Castle E, Bluebond-Langner R, Zhao LC. Coming soon: ability to orgasm after gender affirming vaginoplasty. J Sex Med. 2022;19(5):781–8. https://doi.org/10.1016/j.jsxm.2022.02.015. Epub 2022 Mar 22 PMID: 35337785.
Schardein JN, Nikolavsky D. Sexual functioning of transgender females post-vaginoplasty: evaluation, outcomes and treatment strategies for sexual dysfunction. Sex Med Rev. 2022;10(1):77–90. https://doi.org/10.1016/j.sxmr.2021.04.001. Epub 2021 Jul 1 PMID: 34219008.
Huang JB, Lai A, Morgantini LA, Smith JB 3rd, Millman AL, Cedeno JD, Crivellaro S, Acar O, Kocjancic E. Gender-affirming vaginoplasty: technical considerations in patients with genital skin deficiency. Neurourol Urodyn. 2023;42(5):947–55. https://doi.org/10.1002/nau.25091. Epub 2022 Nov 15 PMID: 36378843.
Robinson IS, Blasdel G, Bluebond-Langner R, Zhao LC. The Management of intra-abdominal complications following peritoneal flap vaginoplasty. Urology. 2022;164:278–85. https://doi.org/10.1016/j.urology.2022.01.036. Epub 2022 Feb 10 PMID: 35150666.
Castanon CDG, Matic S, Bizic M, Stojanovic B, Bencic M, Grubor N, Pusica S, Korac G, Djordjevic ML. Laparoscopy assisted peritoneal pull-through vaginoplasty in transgender women. Urology. 2022;166:301–2. https://doi.org/10.1016/j.urology.2022.05.001. Epub 2022 May 10 PMID: 35550383.
Dy GW, Salibian AA, Blasdel G, Zhao LC, Bluebond-Langner R. External genital revisions after gender-affirming penile inversion vaginoplasty: surgical assessment, techniques, and outcomes. Plast Reconstr Surg. 2022;149(6):1429–38. https://doi.org/10.1097/PRS.0000000000009165. Epub 2022 Apr 15 PMID: 35426889.
Dy GW, Sun J, Granieri MA, Zhao LC. Reconstructive Management Pearls for the Transgender Patient. Curr Urol Rep. 2018;19(6):36. https://doi.org/10.1007/s11934-018-0795-y. PMID: 29644476.
Dy GW, Dugi DD, Peters BR. Skin Management during robotic peritoneal flap vaginoplasty for penoscrotal hypoplasia secondary to pubertal suppression. Urology. 2023;173:226–7. https://doi.org/10.1016/j.urology.2022.12.020. Epub 2022 Dec 30 PMID: 36592702.
Parker A, Brydges H, Blasdel G, Bluebond-Langner R, Zhao LC. Mending the gap: alloderm as a safe and effective option for vaginal canal lining in revision robotic assisted gender affirming peritoneal flap vaginoplasty. Urology. 2023;173:204–8. https://doi.org/10.1016/j.urology.2023.01.003. Epub 2023 Jan 13 PMID: 36642117.
Salibian AA, Schechter LS, Kuzon WM, Bouman MB, van der Sluis WB, Zhao LC, Bluebond-Langner R. Vaginal canal reconstruction in penile inversion vaginoplasty with flaps, peritoneum, or skin grafts: where is the evidence? Plast Reconstr Surg. 2021;147(4):634e–43e. https://doi.org/10.1097/PRS.0000000000007779. PMID: 33776039.
Author information
Authors and Affiliations
Contributions
EH, SA, and MF wrote the main manuscript text. MF prepared the figure. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
All reported studies involving human participants were in accordance with the ethical standards of institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Haile, E., Agrawal, S. & Fascelli, M. Peritoneal Vaginoplasty in Gender Diverse Patients. Curr Obstet Gynecol Rep 13, 136–143 (2024). https://doi.org/10.1007/s13669-024-00389-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13669-024-00389-8